
The Great War was the first truly industrialized war. We saw glimmers of things to come in the years before, with conflicts like the American Civil War and the Franco-Prussian War. However, that paled in comparison to the mechanized destruction brought to the fore by the opening volleys of the First World War. A single day of combat could see tens of thousands dead in a fell swoop. Despite this, it could’ve been a far grislier affair. Medical practices had to keep pace with the ghastly wounds inflicted on soldiers.
The practice of field medicine was forced to evolve, or fighting men would simply be left dead on the operating table. By the time the guns fell silent on the 11th minute of the 11th hour of the 11th day in November of 1918, around 20 million people had died in the wake of the war. A further estimated 21 million were wounded. Against this brutal backdrop, field medicine evolved to lay the groundwork for things like modern surgery, blood transfusion, psychiatric care, and reconstructive practices. The Great War wasn’t simply the War to End All Wars, but the crucible of modern medicine as we know it.
Blood Transfusions
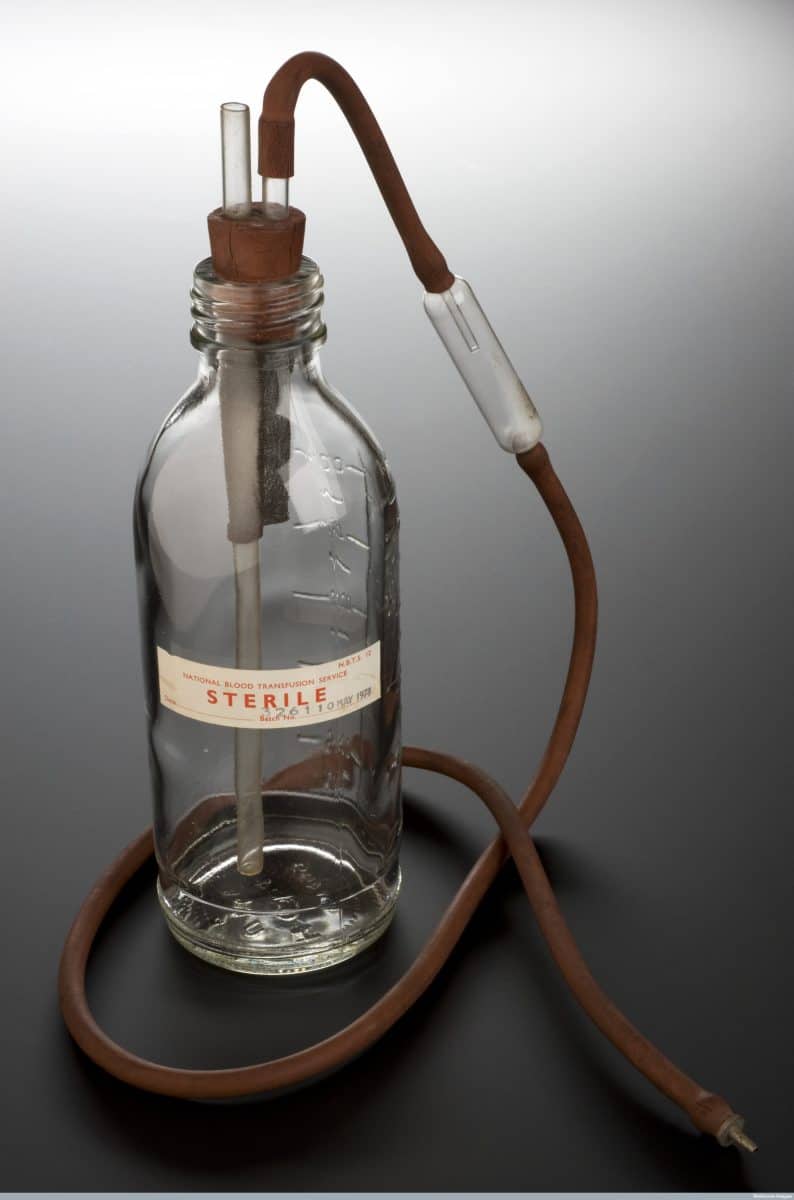
©"Credit- Science Museum, London, Wellcome Images (12655220003)" by Wellcome Images is licensed under BY 2.0. – Original / License
No single advance seen throughout the war has had quite the same impact as the development of a viable blood transfusion. In the years before World War 1, blood transfusions were conducted by directly transferring blood from one person to another. This was a risky move, often resulting in fatal consequences, given a limited understanding of blood types. Blood types were discovered in 1901, thanks to Karl Landsteiner and the ABO System, but the practical application of this discovery wasn’t as quick as you’d expect.
In 1914, that all changed, seemingly overnight. It was discovered that sodium citrate could prevent blood from clotting, enabling a viable storage solution. Transfusion practices changed from a roll of the dice to a genuine possibility to prolong the life of the wounded. In 1917, developments by Dr. Lawrence Bruce Robertson saw transfusions performed all along the Western Front. That same year, American physician Dr. Oswald Robertson pushed this innovation further and developed the first blood bank.
This was a rather crude implementation, at least when taking into account the century of development we’ve had since. Ice-packed containers of O-type blood treated with sodium citrate made it possible for the transport and ultimately practical use of transfusions as a means to guarantee survival. Soldiers who might have died in hours had a new lease on life, often returning home from the front. This very concept, of the modern blood bank, wasn’t devised by idle hands, but rather on the wartorn landscapes of the Western Front.
The Birth of Military Psychiatry

©Ground Picture/Shutterstock.com
We’ve known the effects of combat for centuries, often called battle fatigue. Little was done to treat it in the years before World War 1. Men might even be executed for cowardice or dereliction of duty. The conditions of the Great War saw these effects exacerbated to the extreme. Men were rendered blind, struck mute, or came down with inconsolable nightmares. Early military responses, like those in centuries before, were often ones of contempt.
This came to be known as shell shock, or post-traumatic stress disorder as we know it today. The sheer volume of cases on all sides of the conflict made it impossible to ignore after a point. You could dismiss dozens of people afflicted by it, perhaps, but when tens of thousands of soldiers were struck with it, it isn’t as easy to ignore. An estimated 80,000 British soldiers received psychiatric treatment for PTSD during the war.
The British were a pioneering force in the early days of psychiatric care for the condition. Physicians like Dr. W.H.R. Rivers at the Craiglockhart War Hospital started developing techniques we still use to treat trauma. Talk therapy and targeted trauma-focused treatment were seen as radical ideas at the time. Dr. Rivers would treat famed poet Siegfried Sassoon, documenting his progress every step of the way. World War 1 forced the military establishment to accept that the mind could bear wounds just as severe as those inflicted on the physical body. This shift in thinking seeded the fields of trauma therapy and would later result in clinical recognition of PTSD.
Cosmetic Surgery
Nurse prepare gauze to dressing would.
©Anukool Manoton/Shutterstock.com
The wounds inflicted by the likes of high-explosive artillery, shrapnel, and chemical weapons could maim and disfigure soldiers like nothing seen before. Men would be taken to field hospitals, maimed, often bearing great wounds that were produced at a scale unheard of in previous conflicts. Soldiers were often taken to hospitals with missing jaws, skulls with great chunks gouged out, and grievous wounds to the face with no viable means of repair. Given the previous advances and some aspects we’ll cover, these soldiers often returned home.
Dr. Harold Gillies would rise to the challenge. He would develop techniques for skin grafting, tissue flaps, and facial reconstructive surgery that were shockingly sophisticated for the era. More than 5,000 men would be treated with the techniques he pioneered, often giving these soldiers a semblance of normalcy after their experiences.
Each case was documented, often with photographs and meticulous notes. Techniques like the tubed pedicle graft, which kept a strip of living skin attached to a blood supply before transferring, served as the technical foundation for cosmetic surgery. While often seen as something of an extravagance in the modern era, cosmetic surgery found its footing in the wake of the horrors of World War 1.
Wound Management
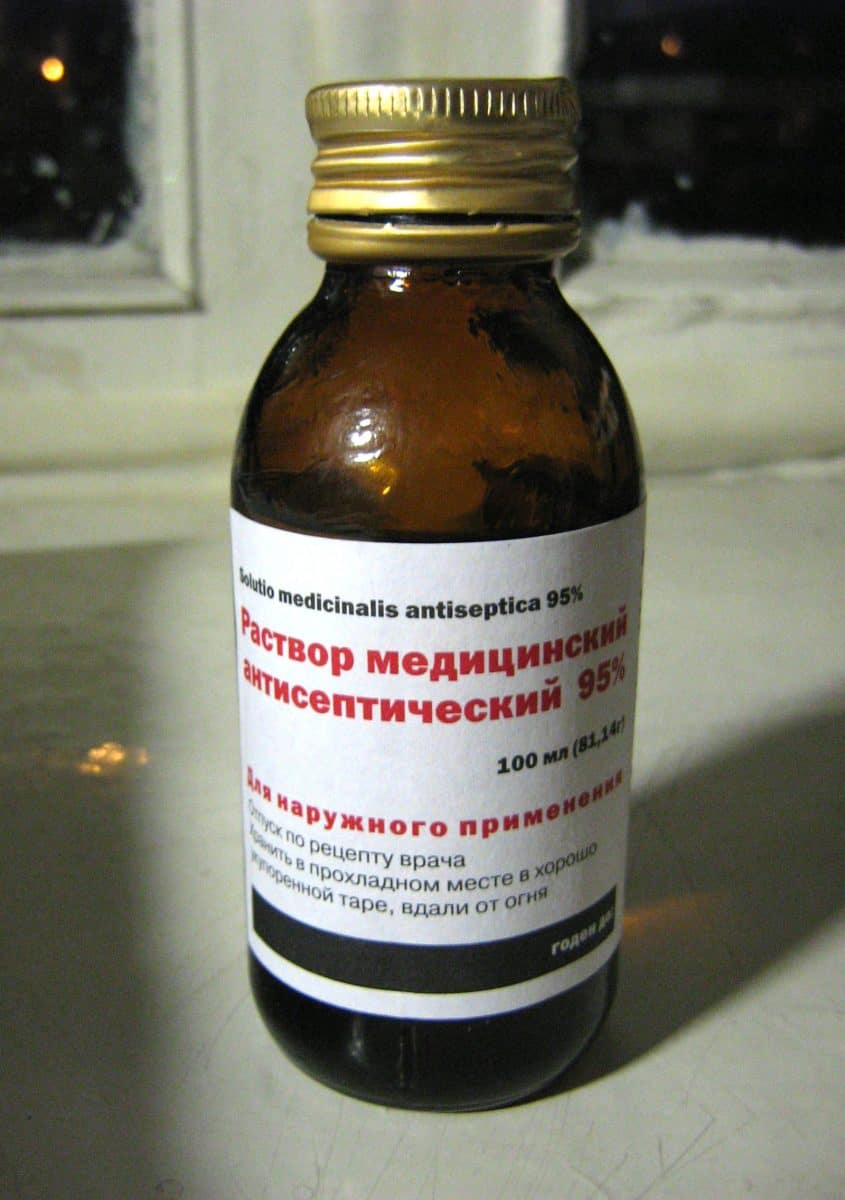
©"Ethanol antiseptic" by VanHelsing.16 is licensed under BY-SA 2.5. – Original / License
The mud and grime of the Western Front presented the potential for dangerous infections. Much of the fighting alongside the French countryside was on arable land, inoculated with manure and other micro-organisms that promoted rich growing conditions. When fresh wounds were exposed to these microbes, bacteria, and fungi, it was the stuff of nightmares. Wounds infected with freshly exposed earth became infected at an alarming rate, and the standard antiseptic of the era, carbolic acid, often resulted in necrotized tissue along withe infection.
French surgeon Dr. Alexis Carrel and British chemist Henry Dakin developed a rather effective response in the Carrel-Dakin method. This utilized a diluted sodium hypochlorite solution, delivered directly to wounds through the use of rubber tubes at regular intervals. It was a time-consuming, cumbersome method of managing wounds, but it was highly effective for the time. Infection rates dropped dramatically when utilizing the Carrel-Dakin method.
In France, Marie Curie, who was already a Nobel laureate for her work in radioactive materials, drove petit Curies, or mobile X-ray stations, to the front. Surgeons could actively locate shrapnel, rather than probing blindly through a wound to find it. An estimated million X-ray examinations were performed throughout the war, saving lives along the way.
Triage

©"Wounded Triage France WWI" by Otis Historical Archives Nat'l Museum of Health & Medicine is licensed under BY 2.0. – Original / License
Before World War 1, there was no systematic method for deciding who received treatment first. It was often down to whoever arrived first, or perhaps who was most horrifically wounded. Given the sheer scope and scale of the wounded arriving at field hospitals, a system needed to be in place. Triage systems were first developed in France by Dr. Antonin Gosset, who had seen the reality of casualty stations.
Systematic, standardized treatment methods were developed, with patients divided into three groups: those who would survive without immediate treatment, those who needed urgent intervention, and those who were too wounded to effectively treatment. This sounds cold, maybe even cruel, but it was the only rational way to save the maximum number of lives with the resources and technical knowledge of the time.
The wounded came in droves, and medical resources were finite. At the end of the day, it was about saving who you could realistically deliver care to, rather than wasting time, resources, and manhours trying to work on a lost cause. The triage system was developed right alongside the battlefield. The same methods of thinking largely haven’t changed when looking at the field hospitals and emergency rooms of today, although they have received some refinements in the century since.
Conclusion
The medical advances seen throughout World War 1 weren’t forged in well-funded laboratories or through peaceful academic inquiry. They came about as a matter of desperation, as the pressure of seeing tens of thousands die as a result of what might have been survivable wounds weighed on care providers. Tirelessly, the physicians, nurses, and scientists at the forefront of these developments did so under a trial by fire, trying to provide care while the great machines of the world raged on.
What was left in the wake of the war, like blood banks and reconstructive surgery, helped lay the foundation for modern medicine as we know it. Every blood transfusion, every patient being triaged, every person treated for trauma, has its roots in World War 1.
The image featured at the top of this post is ©National Library of Scotland / Public Domain – License / Original